

by Julie Santall
Judy’s Story
Judy walked into my room clinging tightly to the arm of her partner. A tall, elegant woman of 69, she appeared frightened, vague and uncertain. She sat down without letting go of him. I noticed immediately her dependence on him and his apparent impatience with that dependence. Each time he shifted away, she reached for him again. Judy had brought him for support, but it quickly became clear that his presence was not helping her feel safe.
Judy had been referred to me by a local wellness clinic. More than ten years earlier, she had been prescribed Cymbalta (duloxetine), a serotonin-norepinephrine reuptake inhibitor (SNRI), by her psychiatrist.
SNRIs are based on the “monoamine hypothesis” of depression. They work by blocking the serotonin transporter (SERT) and norepinephrine transporter (NET), theoretically increasing signalling in parts of the brain involved in mood, attention and pain regulation. However, despite decades of use, the precise mechanisms of antidepressants and antipsychotics remain poorly understood.
Judy had originally been prescribed 30 mg of Cymbalta. Several years earlier she had attempted to discontinue the medication and had successfully reduced to 5 mg. However, she dropped from 5 mg to zero too quickly and experienced severe withdrawal symptoms. Feeling “awful,” she returned to her doctor, who reinstated Cymbalta at 60 mg before later reducing it to 30 mg and adding Lexapro (escitalopram), an SSRI, to “assist” the withdrawal process.
Her pharmacist raised concerns about serotonin syndrome, which caused Judy considerable anxiety. Serotonin syndrome is a potentially serious reaction caused by excessive serotonin activity, usually when multiple serotonergic medications are combined. Ironically, while stopping psychiatric medication too abruptly can be dangerous, adding medications can also create complications.
This uncertainty led Judy to compulsively research her symptoms online using ChatGPT and other sources, which only intensified her fear.
What Judy was actually experiencing was a combination of rapid withdrawal from psychotropic medication, multiple interacting prescriptions, escalating anxiety, poor sleep and eventually akathisia.
Akathisia is a movement disorder characterised by an intense inner restlessness and an overwhelming urge to move. Although not life-threatening, it can be profoundly distressing and may contribute to agitation, despair and suicidal thinking.
Neuroadaptation and Withdrawal
Over the years Judy’s brain had adapted to the medications she was taking. This process, known as neuroadaptation, involves changes in receptor sensitivity and neurotransmitter regulation. When medications are withdrawn too quickly, the nervous system can become destabilised.
Judy had experienced this before. In her twenties, after treatment for anorexia, she had abruptly stopped antidepressants and experienced withdrawal symptoms. Years later, when she attempted to stop Cymbalta rapidly under medical guidance, she again experienced severe withdrawal.
Unfortunately, as often happens, her psychiatrist interpreted the withdrawal symptoms as a relapse of depression or anxiety and reinstated the medication at a higher dose.
Withdrawal vs Relapse
Distinguishing withdrawal from relapse is critical.
Withdrawal symptoms typically begin within days of reducing or stopping medication. They may include:
- dizziness
- nausea
- insomnia
- “brain zaps” or electric shock sensations
- anxiety and agitation
- akathisia
- intrusive or violent thoughts
Withdrawal symptoms often improve if the medication is reinstated to the last stable dose.
Relapse, on the other hand, usually develops gradually over weeks or months and mirrors the original emotional presentation prior to medication. It does not reliably improve with rapid dose increases.
Repeated cycles of withdrawal and reinstatement can also contribute to what is known as kindling.
Kindling
Kindling refers to a phenomenon in which repeated cycles of substance use and withdrawal sensitise the nervous system, causing each withdrawal episode to become more severe.
Historically associated with alcohol and benzodiazepines, kindling is now increasingly recognised in psychotropic drug withdrawal. Over time the nervous system becomes more reactive, increasing sensitivity to future reductions and making withdrawal progressively harder to tolerate.
Polypharmacy and Nervous System Overload
By the time Judy came to see me, she was experiencing severe anxiety, cognitive impairment and insomnia.
Her psychiatrist had prescribed propranolol, a beta blocker often used to reduce physical symptoms of anxiety. When Judy reported ongoing insomnia, she was then prescribed olanzapine, an antipsychotic medication commonly used for sedation at low doses.
The olanzapine caused significant morning sedation, so dexamphetamine was added to counteract the grogginess.
At this point, multiple medications with opposing effects were interacting in her system simultaneously:
- Cymbalta
- Lexapro
- propranolol
- olanzapine
- dexamphetamine
The result was increasing agitation, anxiety and nervous system dysregulation.
If I were to fully explain the pharmacological interactions between these drugs, it would require another article entirely. Suffice to say, it was clear why Judy’s nervous system was in such distress.
Judy’s History
Judy explained that in 2008 she had been working as a social worker in an adolescent mental health unit while raising four adopted children on her own, one of whom was autistic and required intensive care.
She had never married. Work became a way of escaping the overwhelming responsibilities at home.
She also described a childhood in which she had acted as her mother’s confidant and emotional support. Between the ages of 16 and her early twenties she had struggled with anorexia and had previously been prescribed antidepressants.
To manage the overwhelm in adulthood, Judy increasingly relied on red wine. Eventually she entered a detox program, where she met the psychiatrist who first prescribed Cymbalta.
Even before our work together began, Judy had already experienced one failed taper. Following standard pharmaceutical guidelines suggesting that withdrawal effects are mild and self-limiting, her psychiatrist reduced her rapidly from 60 mg to 30 mg.
This history was significant because it suggested a sensitised or “kindled” nervous system. I knew she would likely require a very gradual taper to minimise further harm.
Dependence vs Addiction
The terms dependence and addiction are often used interchangeably, but they describe different phenomena.
Dependence
Dependence is primarily physiological. The body adapts to the presence of a substance and begins to rely on it to function normally.
Characteristics of dependence include:
- tolerance
- withdrawal symptoms when stopping
- neuroadaptation within the nervous system
A person can be dependent without being addicted. For example, someone prescribed opioid medication for severe pain may develop physical dependence without compulsive misuse.
Addiction
Addiction is behavioural and psychological. It involves compulsive use despite harmful consequences.
Characteristics of addiction include:
- loss of control
- compulsive cravings
- continued use despite harm
- psychological reliance to manage emotional pain
From an Internal Family Systems (IFS) perspective, addictive behaviours can be understood as protective “firefighter” parts attempting to numb distress or emotional overwhelm.
In Judy’s case, her primary issue was dependence rather than addiction. Her brain had adapted to long-term exposure to psychotropic medication.
The Brain’s Adaptation to Medication
With antidepressants and antipsychotics, the brain adapts to the constant presence of the drug.
The widely promoted “chemical imbalance” theory of depression has been increasingly challenged in recent years. Critics argue that the theory was oversimplified and heavily marketed by pharmaceutical companies.
The brain continually strives for homeostasis. In response to ongoing medication exposure, receptor sensitivity changes and neurotransmitter systems recalibrate.
Over time the nervous system becomes dependent on the presence of the medication.
This is why reducing psychiatric medication can become so difficult.
Hyperbolic Tapering
Judy wanted to discontinue her medication safely. Given her history, I believed she would need to taper hyperbolically.
Hyperbolic tapering involves making progressively smaller reductions as the dose becomes lower.
Rather than reducing linearly — for example by dropping 10 mg each time — reductions become increasingly gradual near the end of the taper.
For example:
- 40 mg → 20 mg
- 20 mg → 10 mg
- 10 mg → 5 mg
- 5 mg → 2.5 mg
Another common approach is reducing by approximately 10% of the previous dose and holding for periods of stabilisation between reductions.
Why Hyperbolic Tapering Matters
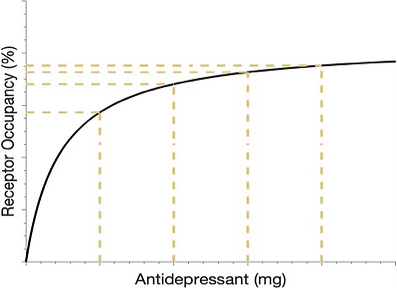
Research using receptor occupancy studies suggests that even low doses of antidepressants can occupy a very high percentage of brain receptors.
This means that small reductions at lower doses may have disproportionately large effects on the nervous system.
In practice, this is why dropping from 5 mg to zero can feel far more destabilising than reducing from 40 mg to 35 mg.
Psychiatrists and researchers such as Mark Horowitz and David Taylor discuss this extensively in The Maudsley Deprescribing Guidelines (2024). Anders Sørensen also explores these principles in Crossing Zero (2025).
The Emotional Dimension
Judy had spent much of her life moving away from painful emotions through work, wine and eventually medication.
This is profoundly human. Most of us seek relief from emotional pain.
However, tapering medication often means that long-suppressed emotions begin to surface again.
The therapeutic task is not simply medication reduction. It is helping the client build the capacity to tolerate and understand difficult emotional and bodily experiences.
Antidepressants can dampen emotional intensity, but they do not resolve the underlying life experiences, attachment wounds or unresolved trauma contributing to suffering.
Judy had never truly stopped to examine:
- why she adopted four children while still very young and living at home
- why she developed anorexia at sixteen
- why she relied so heavily on work and caretaking
- why she felt unable to tolerate stillness or emotional discomfort
Eventually, her attempts to numb overwhelm resulted in dependence on a complex medication regimen that caused significant iatrogenic harm.
A Kindled Nervous System
Judy’s tapering journey has been difficult.
Despite collaborative planning with her integrative doctor and myself, she struggled to follow the tapering schedule consistently. Feeling temporarily stable after an initial reduction, she reduced again too quickly.
Her nervous system reacted intensely.
Once a nervous system becomes highly sensitised or kindled, even minor changes — including supplements or seemingly benign medications — can trigger significant symptoms.
At that point, there is often no medication that can simply “fix” the problem. The work becomes learning how to gradually tolerate and regulate bodily sensations rather than constantly escaping them.
Judy also developed cognitive difficulties after multiple medication changes and additions.
Compounding matters further, her partner responded with frustration and criticism rather than emotional safety. From an attachment perspective, this lack of safety likely amplified her nervous system distress.
When overwhelmed, Judy repeatedly sought reassurance from her psychiatrist, whose primary response was further medication changes.
As the saying goes: when your only tool is a hammer, every problem begins to look like a nail.
The Role of Counselling
My primary focus with clients withdrawing from substances or psychotropic medications is resourcing.
In practical terms, this means helping them find even brief moments of safety, steadiness or calm within the body and mind.
Only when the nervous system has some degree of stability can deeper therapeutic work occur.
The goal is not merely to remove medication, but to help clients understand themselves more deeply rather than relying solely on substances or compulsive behaviours to manage distress.
Judy’s story is ongoing.
I hold hope for her because I have seen many people successfully taper from psychiatric medication when the process is gradual, collaborative and carefully supported.
I am one of them.
Her story highlights both the potential dangers of rapid psychotropic withdrawal and the importance of compassionate, informed care.
While her experience is extreme, it is not hopeless.
Every tapering journey is individual. With appropriate pacing, support and nervous system regulation, many people can successfully reduce or discontinue psychiatric medication.
References
Horowitz, M., & Taylor, D. (2024). The Maudsley Deprescribing Guidelines. Wiley Blackwell.
O’Brien, C. P., Volkow, N., & Li, T.-K. (2006). What’s in a word? Addiction versus dependence in DSM-V. American Journal of Psychiatry, 163(5), 764–765.
Sørensen, A. (2025). Crossing Zero. North and Vale.
In his book ‘Crossing Zero’ (2025), Anders Sorenson explains the receptor occupancy/dose relationship. For example, at only 20mg of Prozac – 86% of the brain’s receptors are occupied with serotonin from the drug. This means that the smaller the dose the greater the impact it has on the brain. Mark Horowitz and David Taylor also describe this in their comprehensive book ‘The Maudsley Deprescribing Guidelines’ (2024)
Whitaker, R. (2010). Anatomy of an Epidemic. Crown Publishing Group.
In his book “Anatomy of an Epidemic” (2010) Robert Whitaker summarises a World Health Organisation study (1998) showing that people diagnosed and treated with psychiatric medication for depression had worse outcomes than those not exposed to drugs.
Mark Horowitz interview on withdrawal, relapse and hyperbolic tapering:
In this interview Mark Horowitz discusses the difference between withdrawal and relapse, the effects of long-term antidepressant use and the role of clinicians and peer support in de prescribing and hyperbolic tapering.
Further Reading
Farmer, Adele ‘What I have learnt from helping thousands of people taper off antidepressants and other psychotropic medications’ https://pmc.ncbi.nlm.nih.gov/articles/PMC7970174

